Congenital adrenal hyperplasia occurs as a result of gene mutation.
This results in defective glucocorticoid & mineralocorticoid synthesis.
Excellent Power point explaining congenital adrenal hyperplasia is here
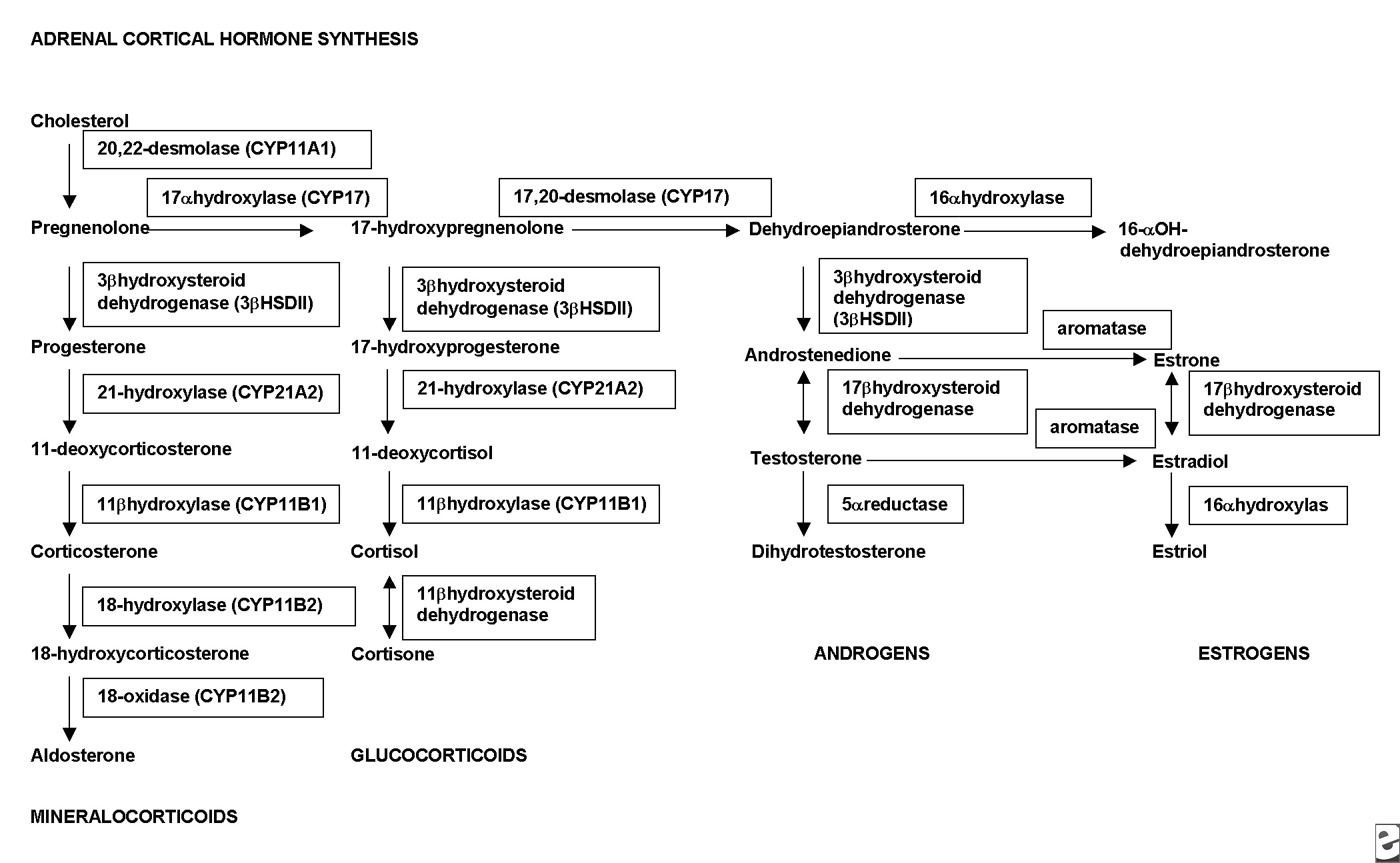
Diagram explaining adrenal hormone synthesis
Mode of inheritance is autosomal recessive.
Clinical features
3 catergories of diseasse - depending on the type of mutation
(I)Salt Wasting(SW)
(II) Simple Virilising(SV)
(III) Non-Classic(NC)
(A) Female infant-ambigious genetalia
(B)Acute illness due to hyponatraemia (salt losing crisis due to mineralocorticoid defeciency)
90% due to 21 hydroxylase enzyme deficiency.These patients have both glucocorticoid & mineralocorticoid defeciency.
5-8% due to 11 hydroxylase deficiency.These patients have excess deoxycortisol, that shows mineralocorticoid activity,leading to hypertension.
How the disease affect pregnancy?
(A)Reduction in fertility , especially in patients with salt wasting type disease.
Reasons: (i) inadequate control of hyperandrogenism
(ii)Inadequate introitus due to poor surgical repair
(B) Disease inheritance by fetus
(C) Risk of Miscarriage,pre-eclampsia & IUGR increased
(D) Masculinization can lead to android type pelvis that may lead to failure to progress in labour.
Management
Antenatal
2 Types of Clical problems
(I) Pregnant women with Congenital adrenal hyperplasia
(II)Women who is carrier for Congenital adrenal hyperplasia with previously affected child( or with a heterozygous partner)
Genetic counselling
(I) This is a autosomal recessive disorder.
(II)Prenatal diagnosis is possible with a battery of gene probes through chorionic villus sampling at 10 weeks
(III) In the past diagnosis made by estimation of 17 hydroxy progestrone & androgen levels in amniotic fluid.
(IV)Zygosity of partner for Congenital adrenal hyperplasia gene can be done.In case gene deletion ,30% of heterozygous , diagnosis can be made accurately.The other 70 % has gene mutation which can be mimicked by pseudo genes of normal individuals. So negative gene testing in the partner reduces the probability of heterozygosity from 1:50 to 1:70.
Differentiation of female genitalia occurs between 9-10 weeks,so even a diagnosis at 10weeks would be late in preventing masculinization of a female fetus with congenital adrenal hyperplasia.
Dexamethasone,the steroid which is capable of crossing the placenta, can be used to suppress the fetal adrenal gland to avoid masculinization. The therapy should be started at least by the fifth week.It may even be started preconceptually. This treatment regime isn't always successful in preventing masculinisation.
Maternal compliance is shown by reduced urinary cortisol or oestriol level.
If the chorionic villus sampling shows a female fetus with congenital adrenal hyperplasia(CAH), the treatment should be continued till delivery.In case of female fetus with congenital adrenal hyperplasia ,termination is also an option.
In a pregnancy with CAH in a male fetus or unaffected fetus the treatment should be discontinued.
Fetal sex determination by ultra sound scan is helpful as maternal androgen excess has minimal effects on male fetus.
Pregnant women with congenital adrenal hyperplasia
On the other hand some steroids can cause masculinization but patients need steroid to suppress their disease activity.However the placental aromatase activity is sufficient to prevent masculinization of fetus.
Hydrocortisone, cortisone acetate, prednisone, methylprednisolone are inactivated in the placenta but dexamethasone crosses the placenta and causes neonatal adrenal suppression.
Regular assessment of clinical status,serum electrolytes and serum androgen levels to adjust the glucocorticoid and mineralocorticoid therapy.
Generally the patients with 21-hydroxylase deficiency doesn't require alteration in dosage during pregancy.
Serum testosterone & free testosterone levels should me measured every 6 weeks in first trimester & every 8 weeks thereafter.Aim is to maintain free testosterone levels at high to normal levels for pregnancy.
Labour & delivery
Elective caesarean is indicated in patients who had genital reconstructive surgery.
Caesaren section rate among these patients is increased and this could be attributed to android type pelvis resulting from masculinization.
Stress dose glucocorticoid therapy ( Hydrocortisone 100 mg IM ) is indicated for patients undergoing labour.
Newborn should be examined for ambiguous genitalia.Female pseudohermaphroditism is either due to maternal hyperandrogenism or fetal 21 hydroxylase deficiency(if father is a carrier).
Affected fetuses would require steroid treatment but even the unaffted fetus would require short term steroid support when its adrenal activity is suppressed in utero as the result of treatment of mother.
Source
1.Nelson-Piercy C. Handbook of obstetric medicine. Taylor & Francis; 2002.
2.Swiet MD. Medical disorders in obstetric practice. Wiley-Blackwell; 2002.
3.1.E.Medicine
4.K. Hagenfeldt , P.O. Janson , G. Holmdahl , H. Falhammar , H. Filipsson , L. Frisén , M. Thorén , and A. Nordenskjöld
Fertility and pregnancy outcome in women with congenital adrenal hyperplasia due to 21-hydroxylase deficiency Hum. Reprod. Advance Access published on July 1, 2008, DOI 10.1093/humrep/den118.Hum. Reprod. 23: 1607-1613.


{kind=link}